Gestational Diabetes – Whats all the fuss?

Author: Claire Wyborn – February 2024
A Gestational Diabetes Mellitis (GDM) diagnosis when you are between 24 to 28 weeks pregnant can completely rock your world, and not in a good way. Lately, there seems to be an increase in healthy women being over diagnosed with gestational diabetes. By “over diagnosed” I mean that their results are borderline on their GDM test.
When some simple, but maybe challenging, changes are made to a more balanced and nutritious approach to their diet, and lifestyle their blood glucose levels remain low. So the question arises… Do you really have GDM if it is diet controlled?
A Gestational Diabetes test is strongly encouraged between weeks 24-28, most often around the time when you have just begun to feel a lot better if you have been challenged with morning/all day sickness. (And often when you are wanting to finish that tub of ice cream or block of chocolate) It may come as a complete surprise to test positive for Gestational Diabetes. Unfortunately, there is not a lot of preparation or conversation prior to offering you the GDM test. Nutrition is glossed over, and definitely not a focal point during short antenatal visits. There is not a lot of education about eating a healthy, wholefood and nutritious diet, especially around the time the GDM test is scheduled.

GDM impacts around 10 – 15% of pregnancies in Australia. A study published in the Medical Journal of Australia, indicates that in Australia we may need to revisit the diagnostic criteria of GDM, this points to evidence that there needs to be a serious revision of the one size fits all approach to testing for GDM.
So what is GDM, what causes it, how does it impact your pregnancy, what are the myths surrounding this concern and what can you do about it?
Our bodies make a hormone called insulin, this helps to keep the glucose in our blood at a good level, if the sugar intake and the insulin balance is out, then a GDM diagnosis is almost certain. During pregnancy there are also hormones that may impact the production of insulin. Unfortunately some ethnicities can be more susceptible to gestational diabetes. This can often be unavoidable, and frustrating.
The challenge many women face is, once you have tested positive for GDM, then sadly antenatal visit are trumped by conversations encouraging early induction, to prevent birthing a big baby. This added stress is also not conducive to a enjoyable pregnancy. The diet restrictions can also be challenging, especially if it is not easy for you to make choices around exercise and healthy eating habits.
- Gestational diabetes is permanent – Not true – your blood sugar levels should settle after your baby is born. Potential lifelong consequences exist for mother and baby if the condition goes untreated; however, adverse maternal and fetal effects can be ameliorated by effective pregnancy management. This includes attention to better nutrition, and in some cases, diabetes medication.
- You must be induced early to prevent your baby being too big at birth – This is a tricky one. Gestational diabetes, that is poorly managed may impact the birth weight of your baby. Many women who do not have GDM can also grow and birth big babies, it cannot be a one size fits all approach. Many believe that if you have GDM then you will grow a huge 4+kg baby – and birth will be difficult. BUT if you have been able to manage your blood glucose levels and they have remained under the threshold….. do you actually have GDM and all the pressure to induce may not actually be accurate or true.
- You need to be on medication when diagnosed with GDM – not completely true – if your blood glucose levels remain under the threshold – (5.1) then do you really have gestational diabetes?
- GDM only affects overweight people – not true – many slim women have been shocked with a GDM diagnosis.
- There is nothing I can do to change the diagnosis – also not true – There is so much you can do to remain healthy, to keep your blood glucose levels (BGL) low.

- Regardless of a GDM diagnosis, there is good evidence that a highly nutritious diet, of mainly whole foods, a great variety of fresh fruit and vegetables, whole grains, healthy fats, and adequate protein is essential when pregnant. Avoid the fast and easy foods that are nutritionally empty and carbohydrate heavy.
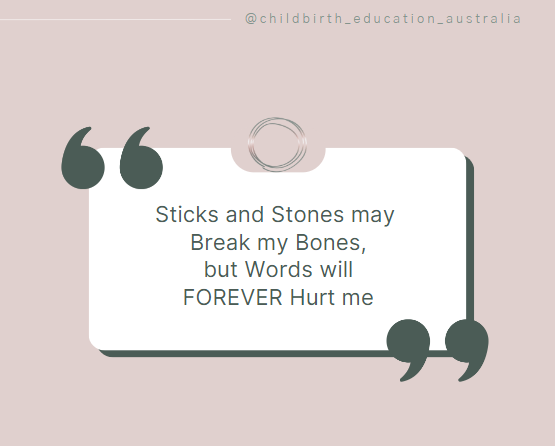
Become an active participant in your pregnancy, do some good research, when you are informed, you are able to make better decisions that feel right for you. Ask questions, be involved with how your pregnancy and birth unfolds.
Resources for further education:
Lilly Nicols has a great website and recipe books for guidance.
Sarah Wickham has an interesting study on induction for GDM and the research surrounding GDM diagnosis and birth outcomes.
References:
- https://www1.racgp.org.au/newsgp/clinical/new-call-to-review-gestational-diabetes-screening
- https://ranzcog.edu.au/wp-content/uploads/2022/05/Diagnosis-of-Gestational-Diabetes-Mellitus-GDM.pdf
- https://www.health.qld.gov.au/__data/assets/pdf_file/0021/370074/diab_gdm_colour.pdf


Responses